Topographic anatomy of the human diaphragm. Diaphragm: structure and function
Diaphragm, diaphragma, represents a squamous muscle, m. phrenicus, dome-shaped curved, covered above and below with fascia and serous membranes. Its muscle fibers, starting around the entire circumference of the lower aperture of the chest, pass into tendon distension occupying the middle of the diaphragm, centrum tendineum... At the place of origin of fibers in the muscular section of the abdominal obstruction, the lumbar, costal and sternal parts are distinguished.
Lumbar part, pars lumbalis, consists of two parts (legs) - right and left, crus dextrum et sinistrum.
Both legs of the diaphragm leave between themselves and the spinal column a triangular gap, hiatus abrticus, through which the aorta passes with the one lying behind it ductus thoracicus... The edge of this hole is bordered by a tendon strip, so that the contraction of the diaphragm is not reflected in the lumen of the aorta. Rising up, the legs of the diaphragm converge with each other in front of the aortic opening and then diverge somewhat to the left and upward from it, forming a hole, hiatus esophageus, through which the esophagus and accompanying both nn pass. vagi.
Hiatus esophageus is bordered by muscle bundles that play the role of a pulp that regulates the movement of food. Between the muscle bundles of each of the legs of the diaphragm, gaps are formed through which nn pass. splanchnici, v. azygos (v. hemiazygos on the left) and the sympathetic trunk.
Costal part, pars costalis,starting from the cartilage of the VII-XII ribs, ascends towards the tendon center.
Sternum, pars sternalis, departs from the posterior surface of the xiphoid process of the sternum to the tendon center. Between pars sternalis and pars costalis there is a paired triangular slit near the sternum, trigonum sternocostalthrough which the lower end penetrates a. thoracica interna (a. epigastrica superior).
Another pair of large slit, trigonum lumbocostal, is between pars costalis and pars lumbalis... This gap, corresponding to the communication existing in embryonic life between the chest and abdominal cavity, is covered from above by the pleura and fascia endothoracica, and below - fascia subperitonealis, retroperitoneal tissue and peritoneum. The so-called diaphragmatic hernia can pass through it.
Somewhat posteriorly and to the right of the midline in the tendon center is a quadrangular opening, foramen venae cavae, through which the inferior vena cava passes. As indicated, the diaphragm has a domed shape, but the height of the dome is asymmetrical on both sides: its right side, supported from below by a bulky liver, is higher than the left.
Function. The diaphragm contracts with inhalation, the dome flattens, and it descends. Due to the lowering of the diaphragm, an increase in the chest cavity in the vertical direction is achieved, which takes place during inhalation. (Inn. CIII-V N. phrenicus, VII-XII nn. Intercostales, plexus solaris.)
1. Diaphragm: structure, parts, openings, blood supply and innervation. Weak spots
2. Heart (topography, projection on the anterior valve wall, coronary arteries)
3. Auxiliary apparatus of the eye (structural features, functions). Innervation of the lamellar gland
1. Diaphragm: structure, parts, openings, blood supply and innervation. Weak spots. Diaphragm - an unpaired broad muscle that separates the chest and abdominal cavities, which serves to expand the lungs. Conventionally, its border can be drawn along the lower edge of the edges. It is formed by a system of striated muscles, which, apparently, are derivatives of the rectus abdominis muscle system. It is peculiar only to mammals. In the diaphragm, the lumbar, costal and sternal parts are distinguished. Between the lumbar and costal parts there are lumbar-costal triangles, between the costal and sternum - sterno-costal, these formations are the place of occurrence of diaphragmatic hernias. The lumbar part of the diaphragm (pars lumbalis diaphragmatis) begins on the front surface of the bodies of the lumbar vertebrae. The costal part (pars costalis diaphragmatis) begins on the inner surface of the lower six to seven ribs. The sternal part (pars sternalis diaphragmatis) of the diaphragm is the narrowest and weakest, begins on the posterior surface of the sternum. Thus, the muscle bundles of the muscle begin at the periphery, go up and medially and converge with their tendons, forming a tendon center (centrum tendineum). The blood supply to the diaphragm is carried out by the upper and lower diaphragmatic, musculophrenic and pericardial diaphragmatic arteries. They are accompanied by the veins of the same name. The diaphragm is innervated by the phrenic nerve / The functions of the diaphragm are divided into static and dynamic. In dynamic, three separate functions are distinguished: 1. respiratory (or respiratory). As a result of the movements of the diaphragm, which together with the pectoral muscles cause inhalation and exhalation, the main volume of ventilation of the lungs is carried out. cardio-vascular... When you inhale, the heart bag and the lowest part of the superior vena cava lying in it expand. At the same time, a decrease in the diaphragm and a simultaneous increase in intra-abdominal pressure squeeze blood from the liver into the inferior vena cava, which contributes to the constant outflow of venous blood into the right heart. In addition, fluctuations in intrapleural pressure contribute to the outflow of blood from the abdominal organs and its flow to the heart (for example, the suction effect of the chest cavity during inhalation). 3.motor-digestive. The diaphragm is of great importance for the movement of food through the esophagus (it is a pulp of the esophagus), and periodic movements of the diaphragm, coupled with synchronous respiratory movements, are also important for the stomach. The static (supporting) function is to maintain normal relationships between the organs of the thoracic and abdominal cavities, depending on the muscle tone of the diaphragm.
Disruption of this function leads to the movement of the abdominal organs into the chest. The diaphragm is an important abdominal organ. While contracting with the abdominal muscles, the diaphragm helps to reduce intra-abdominal pressure. When you inhale, the diaphragm contracts.2. Heart (topography, projection onto the anterior valve wall, coronary arteries)
In the heart, a base and a top are distinguished. The base of the heart, the basis cordis, faces up, back and to the right. Behind it is formed by the atria, and in front - by the aorta and pulmonary trunk. The rounded apex of the heart, apex cordis, faces downward, forward and to the left, reaching the fifth intercostal space at a distance of 8-9 cm to the left of the midline; the apex of the heart is formed entirely by the left ventricle. The edges of the heart are not the same configuration: the right edge of the heart is sharper; the left one is more blunt, rounded due to the greater thickness of the wall of the left ventricle. Both edges of the heart and part of its posterior-inferior surface are adjacent to the mediastinal pleura and lungs. It is believed that the size of the heart corresponds to the size of a person's fist. Average dimensions of the heart: longitudinal - 12-13 cm, largest diameter - 9-10.5 cm, anteroposterior size - 6-7 cm.In the heart, as in the pericardium, five surfaces are distinguished: sternocostal (anterior), facies sternocostalis (anterior), diaphragmatic (lower), facies diaphragmatica (inferior), two pulmonary (lateral), facies pulmonales (laterales) dextra et sinistra, and posterior, facies vertebralis (posterior). Borders of the heart to the chest wall: * the push of the apex of the heart can be felt 1 cm medially from lineae mamillaris sinistrae in the fifth left intercostal space, * the upper border of the projection of the heart goes at the level of the upper edge of the cartilage of the third ribs. * the right border of the heart runs 2-3 cm to the right from the right edge of the sternum, from III to V rib. * the lower border goes transversely from the cartilage of the V right rib to the apex of the heart, * the left one - from the cartilage of the III rib to the apex of the heart. Listening for valves:mitral - at the apex of the heart, tricuspid - on the sternum on the right against the cartilage of the V rib, the aortic valve - at the edge of the sternum in the second intercostal space to the left of the sternum. The blood supply to the heart is carried out through two main vessels - the right and left coronary arteries, starting from the aorta immediately above the semilunar valves.
Left coronary arteryThe left coronary artery begins from the left posterior sinus of Vilsalva, goes down to the anterior longitudinal sulcus, leaving the pulmonary artery to the right of itself, and to the left - the left atrium and the ear surrounded by fatty tissue, which usually covers it. It is a wide, but short trunk, usually no more than 10-11 mm long. The left coronary artery is divided into two, three, in rare cases into four arteries, of which the anterior descending (LAD) and the circumflex branch (OB), or arteries, are of greatest importance for pathology. The anterior descending artery is a direct continuation of the left coronary.
Along the anterior longitudinal cardiac sulcus, it goes to the apex of the heart, usually reaches it, sometimes bends over it and passes to the posterior surface of the heart.
Several smaller lateral branches depart from the descending artery at an acute angle, which are directed along the anterior surface of the left ventricle and can reach the blunt edge; in addition, numerous septal branches depart from it, piercing the myocardium and branching into the anterior 2/3 of the interventricular septum. Lateral branches feed the anterior wall of the left ventricle and give branches to the anterior papillary muscle of the left ventricle. The superior septal artery gives a branch to the anterior wall of the right ventricle and sometimes to the anterior papillary muscle of the right ventricle. Throughout its entire length, the anterior descending branch lies on the myocardium, sometimes plunging into it with the formation of muscle bridges 1-2 cm long. For the rest of the length, its anterior surface is covered adipose tissue of the epicardium.
The enveloping branch of the left coronary artery usually departs from the latter at the very beginning (the first 0.5-2 cm) at an angle close to a straight line, passes in the transverse groove, reaches the blunt edge of the heart, bends around it, passes to the posterior wall of the left ventricle, sometimes reaches the posterior interventricular sulcus and in the form of the posterior descending artery is directed to the apex. Numerous branches extend from it to the anterior and posterior papillary muscles, the anterior and posterior walls of the left ventricle. One of the arteries supplying the sinoauricular node also departs from it.
Right coronary arteryThe right coronary artery begins in the anterior sinus of Vilsalva. First, it is located deep in the adipose tissue to the right of the pulmonary artery, bends around the heart along the right atrioventricular groove, passes to the posterior wall, reaches the posterior longitudinal groove, and then descends in the form of a posterior descending branch to the apex of the heart. The artery gives 1-2 branches to the anterior wall of the right ventricle, partially to the anterior part of the septum, both papillary muscles of the right ventricle, the posterior wall of the right ventricle and the posterior part of the interventricular septum; the second branch also departs from it to the sinoauricular node.
 ... The diaphragm ... says: "Thanks to me you live, because of me you will die. I hold in my hands the power over life and death; learn to understand me and then you will be calm." A. T. Still
... The diaphragm ... says: "Thanks to me you live, because of me you will die. I hold in my hands the power over life and death; learn to understand me and then you will be calm." A. T. Still
 The diaphragm is a movable tendon-muscular septum between the chest and abdominal cavities. It has a domed shape due to the position of the internal organs and the pressure difference in the chest and abdominal cavities. The convex side is directed into the chest cavity, the concave side is directed downward into the abdominal cavity. The diaphragm is the main respiratory muscle and the most important abdominal organ.
The diaphragm is a movable tendon-muscular septum between the chest and abdominal cavities. It has a domed shape due to the position of the internal organs and the pressure difference in the chest and abdominal cavities. The convex side is directed into the chest cavity, the concave side is directed downward into the abdominal cavity. The diaphragm is the main respiratory muscle and the most important abdominal organ.
 In the diaphragm, the muscle part and the tendon center are distinguished. Muscle bundles come from the periphery, have a muscle or tendon origin. Converging upward from the periphery to the middle of the diaphragm, the muscle bundles pass into the tendon center.
In the diaphragm, the muscle part and the tendon center are distinguished. Muscle bundles come from the periphery, have a muscle or tendon origin. Converging upward from the periphery to the middle of the diaphragm, the muscle bundles pass into the tendon center.
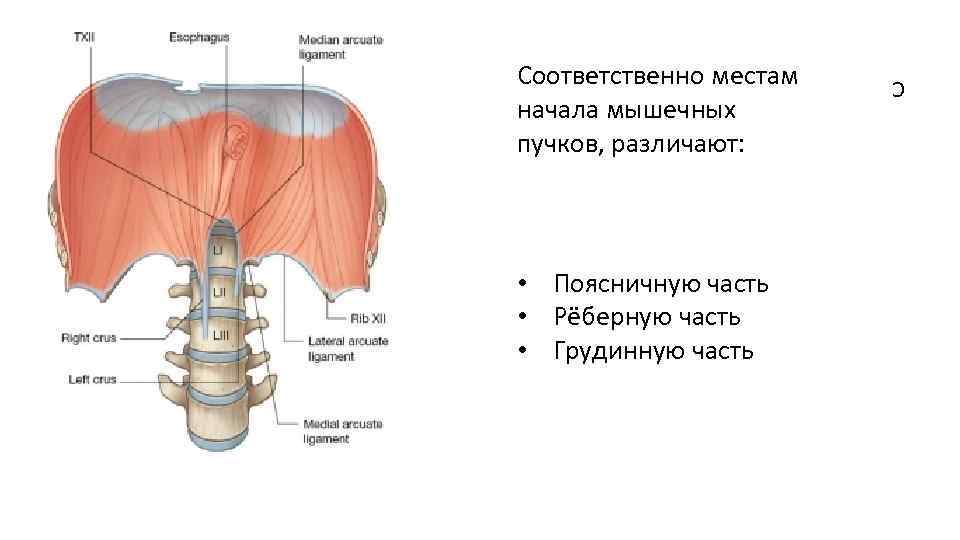 Lumbar part Costal part Sternal part C According to the places where the muscle bundles begin, there are:
Lumbar part Costal part Sternal part C According to the places where the muscle bundles begin, there are:
 The lumbar part starts from the anterior surface of the lumbar vertebrae with three pairs of legs: Medial legs Intermediate legs Lateral legs
The lumbar part starts from the anterior surface of the lumbar vertebrae with three pairs of legs: Medial legs Intermediate legs Lateral legs
 Medial legs The right medial leg is more developed and starts from the bodies L 1 -L 4, and the left leg originates from L 1 -L 3. At the bottom, both legs are woven into the anterior longitudinal ligament of the spine, and at the top their fibers intersect in front of the body L 1, limiting aortic opening. The aorta and thoracic lymphatic duct pass through this opening.
Medial legs The right medial leg is more developed and starts from the bodies L 1 -L 4, and the left leg originates from L 1 -L 3. At the bottom, both legs are woven into the anterior longitudinal ligament of the spine, and at the top their fibers intersect in front of the body L 1, limiting aortic opening. The aorta and thoracic lymphatic duct pass through this opening.

 Medial pedicles The edges of the aortic opening are limited by bundles of fibrous fibers that form the median arcuate ligament. With the contraction of the muscle bundles of the legs of the diaphragm, this ligament protects the aorta from compression, as a result of which there are no obstacles in the path of blood flow in the aorta.
Medial pedicles The edges of the aortic opening are limited by bundles of fibrous fibers that form the median arcuate ligament. With the contraction of the muscle bundles of the legs of the diaphragm, this ligament protects the aorta from compression, as a result of which there are no obstacles in the path of blood flow in the aorta.
 Esophageal opening of the diaphragm Pass the esophagus and vagus nerves. From this zone, Treitz's ligament (muscle) departs to the duodeno-jejunal junction.
Esophageal opening of the diaphragm Pass the esophagus and vagus nerves. From this zone, Treitz's ligament (muscle) departs to the duodeno-jejunal junction.

 Intermediate Legs Are the weakest. They begin lateral to the medial pedicles of the diaphragm from the lateral surface of L 2 and also go to the center.
Intermediate Legs Are the weakest. They begin lateral to the medial pedicles of the diaphragm from the lateral surface of L 2 and also go to the center.
 Lateral legs Originate from the medial and lateral arcuate ligaments and also go to the center
Lateral legs Originate from the medial and lateral arcuate ligaments and also go to the center
 Medial arcuate ligament Stretched over the psoas major muscle between the body L 1 and the apex of its transverse process
Medial arcuate ligament Stretched over the psoas major muscle between the body L 1 and the apex of its transverse process
 The lumbar muscle passes under the medial arcuate ligament of the PPM Association: - kidneys - C 0 -C 1 - Th 11 -12 - emotions: fear of death; sexual indecision - kidney meridian
The lumbar muscle passes under the medial arcuate ligament of the PPM Association: - kidneys - C 0 -C 1 - Th 11 -12 - emotions: fear of death; sexual indecision - kidney meridian
 Lateral arcuate ligament Covers the front of the square muscle of the lower back, throwing over it from the apex of the transverse process L 1 to the 12th rib. Two paired slits remain between the legs of the lumbar diaphragm. The sympathetic trunk passes into the gap between the intermediate and lateral legs.
Lateral arcuate ligament Covers the front of the square muscle of the lower back, throwing over it from the apex of the transverse process L 1 to the 12th rib. Two paired slits remain between the legs of the lumbar diaphragm. The sympathetic trunk passes into the gap between the intermediate and lateral legs.
 Square muscle of the lower back Associations: - large intestine - ileocecal valve - L 2 - emotions: guilt; unworthiness of love - colon meridian
Square muscle of the lower back Associations: - large intestine - ileocecal valve - L 2 - emotions: guilt; unworthiness of love - colon meridian
 On each side of the diaphragm, between the lumbar and costal parts of the diaphragm, there is a triangular-shaped area devoid of muscle fibers - the lumbar-ribbed triangle. Here, the abdominal cavity is separated from the chest cavity only by thin plates of the intra-abdominal and intrathoracic fascia and the serous membranes of the peritoneum and pleura. The same triangular areas are found between the sternum and the costal parts of the diaphragm - the sternocostal triangle. Diaphragmatic hernias may form within these triangles.
On each side of the diaphragm, between the lumbar and costal parts of the diaphragm, there is a triangular-shaped area devoid of muscle fibers - the lumbar-ribbed triangle. Here, the abdominal cavity is separated from the chest cavity only by thin plates of the intra-abdominal and intrathoracic fascia and the serous membranes of the peritoneum and pleura. The same triangular areas are found between the sternum and the costal parts of the diaphragm - the sternocostal triangle. Diaphragmatic hernias may form within these triangles.
 The costal part of the diaphragm It starts from the inner surface of the 6-7 lower ribs with separate muscle bundles that wedge between the teeth of the transverse abdominal muscle. The bundles of muscles of the diaphragm are directed upward and inward and pass into the tendon center.
The costal part of the diaphragm It starts from the inner surface of the 6-7 lower ribs with separate muscle bundles that wedge between the teeth of the transverse abdominal muscle. The bundles of muscles of the diaphragm are directed upward and inward and pass into the tendon center.
 Sternal part of the diaphragm The narrowest and weakest, starts from the posterior surface of the sternum in the region of the xiphoid process.
Sternal part of the diaphragm The narrowest and weakest, starts from the posterior surface of the sternum in the region of the xiphoid process.
 Tendon center The muscle bundles of all parts of the diaphragm, heading towards the center, pass into the tendon center, forming a tendon center that looks like a trefoil. On the front petal of this shamrock lies the heart, and in the right petal there is a quadrangular opening through which the inferior vena cava passes.
Tendon center The muscle bundles of all parts of the diaphragm, heading towards the center, pass into the tendon center, forming a tendon center that looks like a trefoil. On the front petal of this shamrock lies the heart, and in the right petal there is a quadrangular opening through which the inferior vena cava passes.
 The entire diaphragm in a relaxed state has the shape of a beveled spherical bulge facing the chest. Two domes are distinguished in it - right and left. The top of the domes along the parasternal line on the right reaches the level of the 4th intercostal space, and on the left - the 5th intercostal space.
The entire diaphragm in a relaxed state has the shape of a beveled spherical bulge facing the chest. Two domes are distinguished in it - right and left. The top of the domes along the parasternal line on the right reaches the level of the 4th intercostal space, and on the left - the 5th intercostal space.
 The level of standing of the dome of the diaphragm Right Left in the middle. IV rib of the clavicular line in the anterior V rib of the axillary line V rib in the middle VI rib of the axillary line VII rib in the posterior VII rib of the axillary line VIII rib VI rib in the scapular line Seventh intercostal space Eighth intercostal space or VIII rib or IX rib along the paravertebral space Eighth intercostal space Ninth intercostal space line or IX rib or X rib
The level of standing of the dome of the diaphragm Right Left in the middle. IV rib of the clavicular line in the anterior V rib of the axillary line V rib in the middle VI rib of the axillary line VII rib in the posterior VII rib of the axillary line VIII rib VI rib in the scapular line Seventh intercostal space Eighth intercostal space or VIII rib or IX rib along the paravertebral space Eighth intercostal space Ninth intercostal space line or IX rib or X rib
 Diaphragm openings Aortic opening - aorta and thoracic lymphatic duct Esophageal opening - esophagus and vagus nerve Internal arcuate ligament - psoas muscle External arcuate ligament - square muscle of the lower back Between the internal and intermediate legs - celiac nerves, v. azigos on the right and v. hemiazigos on the left. Between the lateral and intermediate legs: sympathetic trunk Opening of the inferior vena cava - in the tendon center Sternocostal triangle: superior epigastric artery and veins
Diaphragm openings Aortic opening - aorta and thoracic lymphatic duct Esophageal opening - esophagus and vagus nerve Internal arcuate ligament - psoas muscle External arcuate ligament - square muscle of the lower back Between the internal and intermediate legs - celiac nerves, v. azigos on the right and v. hemiazigos on the left. Between the lateral and intermediate legs: sympathetic trunk Opening of the inferior vena cava - in the tendon center Sternocostal triangle: superior epigastric artery and veins

 Innervation of the diaphragm Motor nerve phrenic nerve (n.frenicus) Out of C 3 -C 5 (cervical plexus)
Innervation of the diaphragm Motor nerve phrenic nerve (n.frenicus) Out of C 3 -C 5 (cervical plexus)

 Innervation of the diaphragm The phrenic nerve is also a sensory nerve. It innervates the entire posterior surface of the peritoneum, covering the diaphragm, part of the liver and the posterior part of the spleen and pancreas, adrenal glands, gallbladder. Forms anastomoses in the solar plexus.
Innervation of the diaphragm The phrenic nerve is also a sensory nerve. It innervates the entire posterior surface of the peritoneum, covering the diaphragm, part of the liver and the posterior part of the spleen and pancreas, adrenal glands, gallbladder. Forms anastomoses in the solar plexus.

 Innervation of the diaphragm. Vegetative innervation. The parasympathetic innervation of the diaphragm is provided by the vagus nerves. The branches of the solar plexus provide sympathetic innervation.
Innervation of the diaphragm. Vegetative innervation. The parasympathetic innervation of the diaphragm is provided by the vagus nerves. The branches of the solar plexus provide sympathetic innervation.
 Innervation of the diaphragm Thus, the fibers of both legs, which enter the left part of the tendon center, receive innervation from the left phrenic nerve, and those fibers that enter the tendon center on the right are supplied from the right phrenic nerve. The lower 6 or 7 intercostal nerves distribute sensory fibers to the peripheral part of the muscles, the sensory sensitivity of these nerves is confirmed by absolute muscle atrophy on the side of the phrenic nerve destruction.
Innervation of the diaphragm Thus, the fibers of both legs, which enter the left part of the tendon center, receive innervation from the left phrenic nerve, and those fibers that enter the tendon center on the right are supplied from the right phrenic nerve. The lower 6 or 7 intercostal nerves distribute sensory fibers to the peripheral part of the muscles, the sensory sensitivity of these nerves is confirmed by absolute muscle atrophy on the side of the phrenic nerve destruction.
 Diaphragm blood supply Thoracic aorta Abdominal aorta Pericardial diaphragmatic Superior and inferior diaphragmatic Posterior intercostal
Diaphragm blood supply Thoracic aorta Abdominal aorta Pericardial diaphragmatic Superior and inferior diaphragmatic Posterior intercostal

 Neurolymphatic reflex Chapman reflex Full length of the sternum. When this reflex is active, this area is very painful.
Neurolymphatic reflex Chapman reflex Full length of the sternum. When this reflex is active, this area is very painful.

 Emotional connections Depression, constant emotional stress, impracticability of tasks. With an excessive emotional reaction, a person always activates breathing, creating an increased biomechanical load for the diaphragm, which leads to a multidirectional contraction of its muscle fibers.
Emotional connections Depression, constant emotional stress, impracticability of tasks. With an excessive emotional reaction, a person always activates breathing, creating an increased biomechanical load for the diaphragm, which leads to a multidirectional contraction of its muscle fibers.
 Diaphragm development Is laid at the C 4 -C 5 level from the mesoderm. The organs of the chest and phrenic nerve are laid next to it. On the sides - the serophase ligament (future pleuroperitoneal canal). By 8 weeks it moves downward, reaching the level of the chest, and all elements grow together. 8-9 weeks - connective tissue membrane 23 weeks - muscular organ In case of malformations, the pleuroperitoneal canal does not overgrow or hernias are formed due to underdevelopment (non-union) of components.
Diaphragm development Is laid at the C 4 -C 5 level from the mesoderm. The organs of the chest and phrenic nerve are laid next to it. On the sides - the serophase ligament (future pleuroperitoneal canal). By 8 weeks it moves downward, reaching the level of the chest, and all elements grow together. 8-9 weeks - connective tissue membrane 23 weeks - muscular organ In case of malformations, the pleuroperitoneal canal does not overgrow or hernias are formed due to underdevelopment (non-union) of components.


 Respiratory physiology Inhalation 1. Caudal displacement of the diaphragm. Active tension of the muscles located around the circumference of the tendon center. The muscles move away from the fixed base of the lower ribs, lowering the dome of the diaphragm and displacing the abdominal organs caudally. The 12th rib should be well supported by the square muscle of the lower back so that the diaphragm can provide maximum pressure on the abdominal organs.
Respiratory physiology Inhalation 1. Caudal displacement of the diaphragm. Active tension of the muscles located around the circumference of the tendon center. The muscles move away from the fixed base of the lower ribs, lowering the dome of the diaphragm and displacing the abdominal organs caudally. The 12th rib should be well supported by the square muscle of the lower back so that the diaphragm can provide maximum pressure on the abdominal organs.
 Respiratory physiology Inhalation Purpose: active stretching of the lower lobes of the lungs with air. Muscles-stabilizers: scalene, sternocleidomastoid create a fixation point, from which the diaphragm begins to move (prevent the shoulder girdle from shifting downward).
Respiratory physiology Inhalation Purpose: active stretching of the lower lobes of the lungs with air. Muscles-stabilizers: scalene, sternocleidomastoid create a fixation point, from which the diaphragm begins to move (prevent the shoulder girdle from shifting downward).
 Respiratory physiology Inhale 2. Lateral movement - contraction of the external intercostal muscles. Purpose: active stretching of the middle lobes of the lungs with air. Muscles-stabilizers: square muscle of the lower back. The moment the movement of the internal organs reaches its limit, the tendon center becomes a fixation point. The diaphragm raises the lower ribs first, then the upper ribs to expand the chest.
Respiratory physiology Inhale 2. Lateral movement - contraction of the external intercostal muscles. Purpose: active stretching of the middle lobes of the lungs with air. Muscles-stabilizers: square muscle of the lower back. The moment the movement of the internal organs reaches its limit, the tendon center becomes a fixation point. The diaphragm raises the lower ribs first, then the upper ribs to expand the chest.
 Respiratory physiology Inhalation 3. Ventral displacement - contraction of the anterior internal intercostal muscles. Purpose: active stretching of the upper lobes of the lungs with air. Stabilizing muscles: no. The movement is provided by the elasticity of the pericardial-sternal ligaments.
Respiratory physiology Inhalation 3. Ventral displacement - contraction of the anterior internal intercostal muscles. Purpose: active stretching of the upper lobes of the lungs with air. Stabilizing muscles: no. The movement is provided by the elasticity of the pericardial-sternal ligaments.
 Respiratory physiology Exhalation Calm exhalation is passive (the diaphragm relaxes). Forced exhalation involves the accessory muscles of the chest and abdomen.
Respiratory physiology Exhalation Calm exhalation is passive (the diaphragm relaxes). Forced exhalation involves the accessory muscles of the chest and abdomen.


 Structures of the nervous system and large vessels associated with the diaphragm Thoracic sympathetic chain. Solar plexus + visceral nerve, large and small. Intercostal nerves Th 6 - Th 12. The vagus nerve. Abdominal aorta, celiac trunk. Thoracic lymphatic duct.
Structures of the nervous system and large vessels associated with the diaphragm Thoracic sympathetic chain. Solar plexus + visceral nerve, large and small. Intercostal nerves Th 6 - Th 12. The vagus nerve. Abdominal aorta, celiac trunk. Thoracic lymphatic duct.
 Organs Associated with the Diaphragm Internal organs above the diaphragm in the chest. - heart, lungs, esophagus, large vessels. Internal organs that lie below the diaphragm in the abdominal cavity. - kidneys, liver, stomach, pancreas, spleen; large intestine, small intestine.
Organs Associated with the Diaphragm Internal organs above the diaphragm in the chest. - heart, lungs, esophagus, large vessels. Internal organs that lie below the diaphragm in the abdominal cavity. - kidneys, liver, stomach, pancreas, spleen; large intestine, small intestine.

 Clinical manifestations of diaphragm dysfunction. - pain or feeling of tension in the thoracalumbar junction; - pain under the costal arch; - posture disorders; - diseases of the respiratory system (including bronchitis, bronchial asthma, sinusitis); - diseases of the digestive system (the abdominal organs have a direct or indirect, ligamentary connection with the diaphragm)
Clinical manifestations of diaphragm dysfunction. - pain or feeling of tension in the thoracalumbar junction; - pain under the costal arch; - posture disorders; - diseases of the respiratory system (including bronchitis, bronchial asthma, sinusitis); - diseases of the digestive system (the abdominal organs have a direct or indirect, ligamentary connection with the diaphragm)
 Clinical manifestations of the diaphragm Disorders of peripheral circulation in the lower extremities associated with the pathology of the inferior vena cava and abdominal aorta; Lymphoid circulation disorders (including edema of the lower extremities and abdominal edema); Urogenital disorders (the kidneys are in direct connection with the diaphragm). TO
Clinical manifestations of the diaphragm Disorders of peripheral circulation in the lower extremities associated with the pathology of the inferior vena cava and abdominal aorta; Lymphoid circulation disorders (including edema of the lower extremities and abdominal edema); Urogenital disorders (the kidneys are in direct connection with the diaphragm). TO
 Clinical manifestations of diaphragm dysfunctions Instability of L 5 -S 1, which forms a herniated disc Diaphragmatic hernia (heartburn, belching, retrosternal pain) Manifestations of weakness of the quadratus lumbar muscle Manifestations of weakness of the iliopsoas muscle
Clinical manifestations of diaphragm dysfunctions Instability of L 5 -S 1, which forms a herniated disc Diaphragmatic hernia (heartburn, belching, retrosternal pain) Manifestations of weakness of the quadratus lumbar muscle Manifestations of weakness of the iliopsoas muscle
 Pathobiomechanics of the diaphragm. According to L. F Vasilyeva Violations of the abdominal diaphragm in more than 50% of cases are the cause of human diseases. Respiratory failure causes: 1. Vegetative imbalance, squeezing the vagus nerve and disrupting the trophism of organs; 2. Formation of biomechanics of endorhythm of internal organs, ensuring their ligamentous imbalance; Changes the activity of the cranio-sacral rhythm, because each stage of respiration affects the activity of specific bones of the skull. Decrease in the energy activity of the front and rear energy meridians, which leads to the loss of a large amount of energy.
Pathobiomechanics of the diaphragm. According to L. F Vasilyeva Violations of the abdominal diaphragm in more than 50% of cases are the cause of human diseases. Respiratory failure causes: 1. Vegetative imbalance, squeezing the vagus nerve and disrupting the trophism of organs; 2. Formation of biomechanics of endorhythm of internal organs, ensuring their ligamentous imbalance; Changes the activity of the cranio-sacral rhythm, because each stage of respiration affects the activity of specific bones of the skull. Decrease in the energy activity of the front and rear energy meridians, which leads to the loss of a large amount of energy.
 The enlargement of the esophageal opening leads to compression of the cardiac part of the stomach, disrupting its main function - the splitting of complex proteins into simple amino acids, and a person cannot assimilate protein food, with all the ensuing consequences, not to mention the fact that the lumbar-iliac muscle is woven into the legs of the diaphragm and a decrease in its tone leads to nephroptosis. In addition, the diaphragm is influenced by 8 internal organs that attach to it. But the most common problem of imbalance is associated with neck instability, as a result of which the upper cervical spine is blocked and any movement is accompanied by an overload of the mid-cervical spine, constantly compressing the phrenic nerve.
The enlargement of the esophageal opening leads to compression of the cardiac part of the stomach, disrupting its main function - the splitting of complex proteins into simple amino acids, and a person cannot assimilate protein food, with all the ensuing consequences, not to mention the fact that the lumbar-iliac muscle is woven into the legs of the diaphragm and a decrease in its tone leads to nephroptosis. In addition, the diaphragm is influenced by 8 internal organs that attach to it. But the most common problem of imbalance is associated with neck instability, as a result of which the upper cervical spine is blocked and any movement is accompanied by an overload of the mid-cervical spine, constantly compressing the phrenic nerve.

 Types of diaphragm dysfunctions Inspiratory dysfunction - the inspiratory phase is greater than the expiratory phase - 90% Exhalation dysfunction - the expiratory phase is greater than the inspiratory phase -10% Inspiratory dysfunction - 1st degree dysfunction (preservation of the suction action of the diaphragm) 2nd degree dysfunction (without maintaining the suction action) Primary, secondary
Types of diaphragm dysfunctions Inspiratory dysfunction - the inspiratory phase is greater than the expiratory phase - 90% Exhalation dysfunction - the expiratory phase is greater than the inspiratory phase -10% Inspiratory dysfunction - 1st degree dysfunction (preservation of the suction action of the diaphragm) 2nd degree dysfunction (without maintaining the suction action) Primary, secondary
 Diaphragm testing. 4 diagnostic steps. Calm breathing. Forced breathing-dome diagnostics. Forced breathing - rib diagnostics. Diagnostics of the legs of the diaphragm (through the costal-vertebral triangle).
Diaphragm testing. 4 diagnostic steps. Calm breathing. Forced breathing-dome diagnostics. Forced breathing - rib diagnostics. Diagnostics of the legs of the diaphragm (through the costal-vertebral triangle).
 Vertebral-costal triangle Petit or Greenfeld's triangle. SPACE: Under the 12th rib, lateral to the square muscle of the lower back
Vertebral-costal triangle Petit or Greenfeld's triangle. SPACE: Under the 12th rib, lateral to the square muscle of the lower back
 Correction techniques Trigger point correction techniques. Nonspecific dome correction techniques — umbrella technique, axial twisting, inhibition. Specific techniques for correcting one of the domes are for diaphragm dysfunction of 1 and 2 degrees. Correction of the legs of the diaphragm. Correction of the sternum. The final technique is the triangle technique. Fascial techniques.
Correction techniques Trigger point correction techniques. Nonspecific dome correction techniques — umbrella technique, axial twisting, inhibition. Specific techniques for correcting one of the domes are for diaphragm dysfunction of 1 and 2 degrees. Correction of the legs of the diaphragm. Correction of the sternum. The final technique is the triangle technique. Fascial techniques.



The abdominal obstruction or diaphragm delimits the chest cavity from the abdominal cavity. It is divided into two parts: the muscular, pars muscularis diaphragmaticus, and the tendon center, centrum tendineum.
The tendon center of the diaphragm, consists of the anterior leaf, folium anterius, and lateral leaves, folium dexter and folium sinister, located in the horizontal plane, and the muscular part in the vertical plane. The heart is located on the front leaf of the tendon center, the lungs are on the lateral leaves.
Depending on the places of attachment, the muscular part of the diaphragm, in turn, is divided into the sternal part of the diaphragm, pars sternalis, the costal part, pars costalis, and the lumbar part, pars lumbalis.
The legs of the lumbar diaphragm are as follows:
1. Crus mediale - the medial leg starts from the lig. longitudinale anterius and bodies of III or IV lumbar vertebrae on the right; on the left, one vertebra higher. At level I of the lumbar vertebra, both legs converge, limiting the aortic opening for the aorta and thoracic duct.
2. Crus intermedius - intermediate leg - starts from the lateral surface of the body of the II lumbar vertebra and above it passes into the muscular part of the diaphragm.
Z. Crus laterale - lateral leg - starts from the lateral surface of the body of the II lumbar vertebra with the formation of two tendon arcs, is a thickening of the fascia endoabdominalis.
Arcus lumbocostalis medialis - medial lumbar-costal arch - starts from the body of the II lumbar vertebra, spreads over m. psoas major and attaches to the transverse process of the I lumbar vertebra.
Arcus lumbocostalis lateralis - lateral lumbar-costal arch - starts from the transverse process of the I lumbar vertebra, spreads over m. quadratus lumborum and attaches to the XII rib.
Trigonum lumbo-costale - the lumbar-costal triangle is located between the lumbar and costal parts of the diaphragm. Its base is the lower edge of the XII rib. The bottom of the triangle is lined from the side of the chest cavity by the pleura, fused with thin fascial sheets, to which the posterior surface of the kidney and adrenal gland, surrounded by a fatty capsule, is adjacent.
Trigonum sterno-costale - sternocostal triangle lies between the sternal and costal parts of the diaphragm. Its height is from 1.8 to 2.7 cm, the base is from 2.5 to 3 cm.
The diaphragm has the following large holes:
1. Hiatus aorticus - aortic opening - is enclosed between the medial phrenic legs and their tendon part. The aorta and thoracic duct pass through this opening at the level of the XII thoracic vertebra.
2. Hiatus oesophageus - esophageal opening; after the formation of the aortic opening, the medial phrenic legs intersect and, diverging again, form a second opening in the muscular part, the hiatus oesophageus, through which the esophagus and vagus nerves pass. In the lumbar part of the diaphragm there are two holes formed in the form of a figure eight: the lower one is aortic (tendon) and the upper one is esophageal (muscle).
H. Foramen quadrilaterum s. venae cavae inferioris - a four-sided opening of the inferior vena cava - is located in the right leaf of the tendon center of the diaphragm, through which the inferior vena cava passes.
Blood supply to the diaphragm. The anterolateral parts of the periphery of the diaphragm are supplied with blood by aa. intercostales and its front section from aa. pericardiacophrenicae and aa. intercostales. Thus, the system of branches of the descending aorta, thoracic and abdominal parts and subclavian arteries takes part in the roundabout circulation of the diaphragm.
A. phrenica superior supplies blood to the lumbar part of the diaphragm from the side of the chest cavity and the pleura covering it. A. phrenica inferior supplies blood to the diaphragm and peritoneum; the left, in addition, the end of the esophagus, and the right - the wall of the inferior vena cava, the inferior phrenic veins, vv. phrenicae inferioris, adjoining two to the artery of the same name, flow into the inferior vena cava.
Innervation of the diaphragm. N. phrenicus - the phrenic nerve departs from the anterior branches of the III-IV cervical nerves. The left phrenic nerve penetrates the diaphragm and forks on its lower surface; the right one ends with its branches on the upper surface of the diaphragm. 6 lower intercostal nerves take part in the innervation of the posterior diaphragm.
Funnel chest deformity - a congenital defect associated with hyperplasia of cartilage and the lower pairs of ribs themselves. The body of the sternum is displaced posteriorly, forming a depression. The deformity is often asymmetric, the degree of severity of the defect varies greatly. Keel-shaped chest - protruding deformity of the sternum, less common funnel-shaped deformity.
Amastia - pathology of fetal development, as a result of the development of which a person is born without one or both mammary glands. With amastia, breastfeeding becomes impossible and may be accompanied by defects in the ovaries or other body systems, which leads to a disruption in the development of the entire reproductive system. Such a woman has neither breast tissue nor a nipple. Polymastia - the presence of accessory, multiple glands and nipples, representing developed or underdeveloped glands, with clear nipples, located along the "milk line" that runs from the armpits to the inguinal-femoral region. It is more common in women, while the accessory glands during lactation can swell and secrete milk.
Gynecomastia - breast enlargement in men with hypertrophy of glands and adipose tissue. Often there is a painful asymmetrical breast lump that disappears spontaneously. The magnification can be varied. Physiologic gynecomastia occurs in newborns, during puberty, and in older men. There is a pathological form of gynecomastia.
Hernia of the diaphragmatic foramen - protrusion of the esophagus, stomach or small intestine through the diaphragm into the chest cavity. In this case, the work of the esophageal sphincter, which closes the transition from the esophagus to the stomach, is disrupted.
Aplasia of the diaphragm - anomalies in the development of the diaphragm, in which part of the diaphragm or a fragment of any part is missing. In newborns, there is a congenital absence of the entire diaphragm, which is incompatible with life. Allocate unilateral and total aplasia of the diaphragm. Unilateral aplasia can be complete or partial.
Diaphragm relaxation - relaxation of the domes and high standing of the diaphragm, which is based on paralysis, a sharp thinning and persistent displacement of it into the chest with the adjacent organs of the abdominal cavity. Congenital relaxation of the diaphragm is associated with aplasia or underdevelopment of its muscular part, as well as intrauterine trauma or aplasia of the phrenic nerve. Acquired relaxation results from secondary atrophy, damage to the phrenic nerve, or damage to the diaphragm itself by injury or tumor.
DIAPHRAGM (Greek, diaphragma partition; syn. midriff) - a musculo-tendinous septum separating the chest cavity from the abdominal cavity, serving as the main respiratory muscle.
EMBRYOLOGY
D.'s bookmark is carried out in a three-week embryo at the level of the IV-V cervical segment, from it by the 4th week. the transverse septum of His (septum transversum) develops, the edges divides the primary whole (see) into the abdominal and pleuropericardial cavities. Then, from the outer sickle folds located along the lateral sections of the body, pleuroperitoneal membranes (membranae pleuroperitoneales) begin to form, designed to form most of the domes, and the lumbar part of D is formed from the posterior crescent folds. These sections grow forward to the transverse septum, are connected to it, but leave on each side the pleuroperitoneal canal (ductus pleuroperitonealis), which communicates the pleural and abdominal cavities. By the 8th week. there is a fusion of all D.'s bookmarks, edges at this I stage is a connective tissue plate that completely isolates the chest cavity from the abdominal cavity. A derivative of the trunk wall, the secondary costal part (pars costalis), takes part in the formation of a narrow rim along the edge of the diaphragm. In stage II, the connective tissue plate transforms into a tendon muscle formation due to differentiation in place of muscles from myoblasts located in the corresponding D.'s anlages and emanating from III-V or IV-V myotomes. By the 24th week. D. differs from D. of a newborn only in a smaller thickness of muscle fibers.
Arising at the level of the cervical segments, D. gradually moves away from the place of the initial bookmark as the heart and lungs develop, pushing it downward, and by the end of the 3rd month. is located at the level of its usual attachment.
Violation of D.'s bookmarks or their fusion leads to D. developmental defects, such as D.'s congenital absence or its congenital defects. Muscle developmental disorders lead to the fact that D. remains at the connective tissue stage of development, as a result of which the innate relaxation of D. is formed.
ANATOMY
D. is a flat thin muscle (m. Phrenicus), the fibers of a cut, starting around the circumference of the lower aperture of the chest, go up and, converging radially, pass into a tendon extension, forming dome-shaped bulges on the right and left with a depression in the center for the heart (planum cardiacum). Accordingly, in D., the central tendon part (pars tendinea), or the tendon center (centrum tendineum), and the more extensive marginal muscular part (pars muscularis) are distinguished, in a cut three parts are distinguished: sternum, costal and lumbar.
Sternum (pars sternalis) is poorly expressed, consists of several short muscle bundles extending from the inner surface of the xiphoid process of the sternum. The sternum is separated from the costal part by a narrow triangular slit filled with fiber - the sternocostal space (spatium sternocostale) - by Larrey's triangle.
Costal part D. (pars costalis) starts from the inner surface of the cartilage of the VII-XII ribs in separate bundles going up and passing into the tendon center. Triangular slit, Bohdalek's triangle (trigonum lumbocostale) separates the costal part of D. from the lumbar.
Lumbar (pars lumbalis) consists of three legs on each side (tsvetn. fig. 1): outer, intermediate and inner. The outer leg (crus laterale) starts from the outer lumbar-costal arch (areus lumbocostalis med.), Located between the XII rib and the transverse process L 1-2, and the inner lumbar-costal arch (areus lumbocostalis med.), Coming from the body of one of the these vertebrae and attaching to its transverse process. The intermediate leg (crus intermedium) starts from the front surface of the bodies L 2-3, goes up and out, connecting with the fibers of the outer leg, and passes into the tendon center. A sympathetic trunk (truncus sympathicus) passes between the intermediate and external legs, and between the intermediate and internal - on the right the celiac nerves and the azygos vein, on the left - the semi-unpaired vein.
The inner leg (crus mediale) starts from bodies L 3-4 and the anterior longitudinal ligament of the spine. The internal legs, connecting, first form an arch (lig.arcuatum), limiting the opening for the aorta (hiatus aorticus), through a cut also passes the thoracic duct. Behind the aortic opening is limited by the spine.
D.'s esophageal opening (hiatus esophageus) is formed at the expense of the right leg; the left leg takes part in its formation only in 10% of cases.
In the right leg, three muscle bundles are distinguished, of which the right does not take part in the formation of the esophageal opening, and part of the fibers of the middle bundle and the bundle passing to the left side form a muscle loop around the esophagus.
The esophageal opening is a canal with a width of 1.9 to 3.0 cm and a length of 3.5 to 6 cm. The distance between the esophageal and aortic openings is approx. 3 cm, very rarely there is a common esophageal-aortic opening.
Vagus nerves (nn. Vagi) also pass through the esophageal opening of D.
In D.'s tendon center there are three sections: two lateral and front (middle), in which there is an opening for the inferior vena cava (foramen venae cavae s. Quadrilaterum).
Above D. is covered with intrathoracic fascia, pericardium in the zone of the planum cardiacum, as well as the pleura at the point of contact with the lungs and in the zone of sinuses - the diaphragmatic-mediastinal and phrenic-ribbed. The latter is the deepest and reaches 9 cm, but never reaches the level of D. attachment to the ribs, due to which a narrow pre-diaphragmatic space 3-4 cm deep (spatium praediaphragmaticum) is formed, limited by the upper outer surface of D., the inner surface of the ribs, pleura and filled with loose fiber.
The bottom of the D. is covered with an intra-abdominal fascia, over a large extent by the peritoneum, which is absent only between the leaf of the coronary ligament of the liver, around the openings of the esophagus, the inferior vena cava, and on the entire lumbar and last tooth of the costal part of D. The pancreas and the duodenum are adjacent to this retroperitoneal part of D. , as well as the kidneys and adrenal glands surrounded by a fatty capsule. The liver is adjacent to most of the right dome and to the inner section of the left dome, with which the fundus of the stomach and spleen also touch. These organs are connected with D. by means of the corresponding ligaments. The phrenic-esophageal ligament (lig. Phrenicoesophageum), which covers the anterior surface of the esophagus, is of great importance in D.'s hiatal hernias. The lower boundary of D. is stable and corresponds to the place of its attachment, while the position of the domes is very variable and depends on the constitution, age, various patol, processes. Usually the apex of the right dome is at level IV, and the top of the left is at the V intercostal space. When inhaling, D.'s domes descend by 2–3 cm and flatten.

Blood supply carried out by a paired muscular-diaphragmatic artery (a. musculophrenica) from the internal thoracic arteries, the superior phrenic artery (a. phrenica sup.) and the lower phrenic artery (a. phrenica inf.) from the aorta and six lower intercostal arteries (aa. intercostales). The outflow of venous blood occurs through the paired veins running parallel to the arteries, and, in addition, through the azygos vein on the right and semi-unpaired - on the left, as well as through the veins of the esophagus (printing. Fig. 2).
Lymph, vessels D. form, according to various authors, from two (D.A. Zhdanov, 1952) to three (I.N. Matochkin, 1949) and even five networks: pleural, subpleural, intrapleural, subperitoneal, peritoneal (G.M. Iosifov, 1930; M.S. Ignashkina, 1961). D.'s lymphatic vessels play a role in the spread of inflammatory processes from the abdominal cavity to the pleural cavity and vice versa, thanks to the system of limf, vessels that pierce D. They are located mainly along the esophagus, aorta, inferior vena cava and other vessels and nerves passing through D.
The outflow of lymph from D. is carried out from above through the prelateroretropericardial and posterior mediastinal nodes, from below - through the subphrenic: paraortal and paraesophageal.
Innervation... Each half of D. is innervated by the phrenic nerve (n. Phrenicus), branches of the six lower (VII-XII) intercostal nerves and fibers of the phrenic plexus (plexus diaphragmaticus) and solar plexus.
The only motor nerve of the corresponding half of D. is the phrenic nerve, which is formed mainly from the C3-4 roots of the spinal nerves. It has in its composition motor and sensory fibers, which is important in the occurrence of a phrenicus symptom (see). The branches of the lower intercostal nerves are only sensory and vasomotor nerves of a narrow (up to 1-2 cm) peripheral zone of the diaphragm.
PHYSIOLOGY
D. performs two functions: static and dynamic. The static (supporting) function consists in maintaining normal relationships between the organs of the chest and abdominal cavities, it depends on the muscle tone D. Violation of this function leads to the movement of the abdominal organs into the chest.
Dynamic (motor) function is associated with the effect of alternately contracting and relaxing D. on the lungs, heart, and abdominal organs.
As a result of D.'s movements, the main volume of ventilation of the lower lobes of the lungs is carried out and 40-50% of ventilation is carried out in the upper lobes, the edges are provided mainly by the costal-sternal mechanism.
D. during inhalation reduces intrapleural pressure, helping to fill the right heart with venous blood, and pressing on the liver, spleen and abdominal organs, promotes the outflow of venous blood from them, acting like a pump.
D.'s influence on the digestive organs consists of a massaging effect on the stomach and intestines, with a decreased D.'s tone the amount of air in the stomach and intestines increases.
RESEARCH METHODS
With percussion, it is possible to detect a change in the level of D.'s standing or to suspect the movement of the abdominal organs into the chest cavity on the basis of the appearance of zones of dullness and tympanitis above it, in combination with listening to intestinal motility and weakened respiratory noises in this zone.
Changes in position and function of D. are often accompanied by a decrease in the respiratory volume of the lungs (see. Vital capacity of the lungs) and a change in functional respiratory tests, and with changes in the position of the heart - changes in the ECG.
Laboratory data in the diagnosis of D.'s diseases have no independent significance.
X-ray examination is the main objective method for diagnosing injuries and diseases of D. In a direct projection D. is two continuously convex arcs: the top of the right is at the level of the V rib in front, the left one is one rib lower. In a profile study, the front part of D. is located higher, and then it goes backward obliquely down. With calm breathing, D.'s domes descend by 1–2 cm (by one edge), when forcing inhalation and exhalation, D.'s excursion reaches 6 cm.The high standing of both D.'s domes occurs during pregnancy, ascites, and in combination with mobility disorders - with paralytic intestinal obstruction, diffuse peritonitis. The high standing of one of the domes is noted with paralysis and paresis, relaxation of D., large tumors and cysts, liver abscesses, subphrenic abscesses.
Low standing of D.'s domes (phrenoptosis) is noted in asthenic constitution, visceroptosis, defects of the anterior abdominal wall and emphysema of the lungs, and with the latter, limitation of their mobility is also observed.
With paralysis and relaxation of D., a paradoxical movement of the dome can be observed, when it rises when inhaling, and when exhaling, it falls. The nature of D.'s movements and her functional state are examined with the help of special rentgenol, methods. When printing, usually two photographs (diplogram) are made on one film with an exposure of 75% of the usual, first in the D. position on maximum exhalation, and then on inhalation (see Polygraphy).
Single-slit, double-slit or multi-slit X-ray kymography with the use of a special lattice allows you to study the direction, amplitude and shape of the respiratory teeth of D. (see. at X-ray cinematography (see). For targeted studying of details of separate D.'s sections, especially with cysts and tumors, tomography can be applied (see). D.'s position and condition can be indirectly judged by a contrast study of adjacent organs (esophagus, stomach, intestines).
Diagnostic pneumoperitoneum (see), pneumothorax (see artificial pneumothorax) and pneumomediastinum (see Pneumomediastinography) help isolate D.'s image from adjacent organs in the absence of adhesions.
PATHOLOGY
Developmental defects
The most common malformations of D. are non-closure of the pleuroperitoneal canal or impaired fusion of individual D.'s anlages with the formation of congenital false hernias (defects) D. It is very rare that there is a complete absence of a dome or even less often for all D., which is usually incompatible with life. Along with this, congenital underdevelopment of muscle tissue in both or one dome or some of its sections with the development of congenital complete or partial relaxation of D. also occurs. Extremely rare cases of the so-called also belong to malformations. non-omission of D., when the place of its attachment to the chest wall and the spine is located higher than usual.
Damage
They can be divided into open (gunshot, stab-cut) and closed (traumatic); the latter are subdivided into direct, indirect and spontaneous. All thoracoabdominal wounds with damage to internal organs are accompanied by D.'s injuries (see Thoracoabdominal injuries). Occasionally there are isolated wounds of her without damage to the organs adjacent to her. Closed D.'s injuries are encountered during transport injuries and falling from a height. D.'s gap is most often caused by a sudden increase in intra-abdominal pressure, much less often a similar mechanism can be noted with chest injuries, In 90-95% of cases with a closed D.'s injury, its left half is affected; rupture of both domes is very rare. As a rule, there is a rupture of the tendon part of the dome or its separation from the muscle section. Less often, there is a rupture of the lumbar part with damage to the esophageal opening or D.'s separation from the place of its attachment. Direct closed injuries of D. also occur when it breaks with a broken rib. Isolated closed D.'s injuries are also rarely observed, usually they are combined with damage to the pelvic bones and abdominal organs.
Through D.'s rupture, both with open and closed injuries, abdominal organs can fall out into the pleural cavity - more often the stomach, omentum, loops of the large and small intestines. Occasionally, with large tears on the right, the liver may fall out into the defect, and the spleen on the left. Loss can occur both immediately after injury, and after a certain period of time.
Clinical picture usually masked by manifestations of concomitant trauma (pleuropulmonary shock, respiratory and cardiovascular failure, hemopneumothorax, peritonitis, bleeding, bone fractures). Only signs of compression of the lung and displacement of the heart by the abdominal organs displaced into the chest, and especially the symptoms of compression or infringement, are of independent diagnostic value. It is difficult to recognize D.'s damage. An auxiliary sign of thoracoabdominal injury with open injuries is the direction of the wound channel. A reliable diagnosis can be made with open injuries on the basis of the prolapse of the abdominal organs into the chest wound or the outflow of feces and urine from it, as well as the detection of hollow abdominal organs in the chest, if necessary in such cases, as well as with closed injuries, rentgenol , research.
The presence of hemo- or pneumothorax with damage to the abdomen raises suspicion of possible damage to D.
When laparotomy for abdominal trauma or torapotomy in case of damage to the organs of the chest cavity, it is imperative to examine D. to exclude its rupture.

Treatment. With a diagnosed rupture of D., simple suturing is shown (Fig. 1) with separate sutures from non-absorbable suture material after lowering the abdominal organs and excision of non-viable diaphragm tissues through the same access that was used for revision (thoraco- or laparotomy). To strengthen the seams, the formation of a duplication of D. is possible. The need for plastic strengthening of D., as a rule, does not arise, since extensive injuries that give a large defect are usually accompanied by a trauma of adjacent organs that is incompatible with life.
Diaphragmatic hernia
Diaphragmatic hernias represent the movement of the abdominal organs into the chest cavity through a defect or weak area D. They are characterized by the presence of a hernial orifice, a hernial sac and hernial contents. In the absence of a hernial sac, the hernia is called false (hernia diaphragmatica spuria), and if there is one - true (hernia diaphragmatica vera); in these cases, the hernial sac is necessarily covered from below by the parietal peritoneum, and from above by the parietal pleura.
All D.'s hernias are divided, according to the classification of B.V. Petrovsky, N.N. Kanshin, N.O. Nikolaev (1966), into traumatic and non-traumatic.
Non-traumatic hernia, in turn, are divided into false congenital hernias (defects) D., true hernias of weak zones D., true hernias of atypical localizations, hernias of D.'s natural openings - esophageal opening, rare hernias of D.'s natural openings.
Of nontraumatic hernias, congenital hernias (defects) D. are also false, which are often incorrectly called eventrations, they can also be observed in adults.
True hernias of weak zones include parasternal hernias (Fig. 2), which are also referred to as “anterior diaphragmatic hernia”, “retroxifoidal”, “substernal”, “subcostal”, “subcostal”, “Morgagni's hernia”, “Larreya's hernia ". A parasternal hernia can be retrocosternal, emerging through the sternocostal triangle of Larrey, it can be called Larrey's hernia, and retrosternal, associated with underdevelopment of the sternal part of D. Usually, the contents of the hernial sac in parasternal hernias are the omentum and the transverse colon and parasternal gut , in which through the hernial orifice in D., as with a sliding hernia, the preperitoneal fatty tissue protrudes. True hernia of the lumbar-costal triangle is very rare. True hernias of atypical localization are casuistic rarities; they often lack pronounced hernial orifices. Among hernias of natural openings of D., hernias of the esophageal opening are very common and, due to the peculiarities of the anatomical structure, clinical picture and treatment, represent a special group of diaphragmatic hernias. Some cases of rare hernias of other natural openings of D. are described: clefts of the sympathetic nerve, openings of the inferior vena cava.
Traumatic hernia arise as a result of thoracoabdominal wounds and D.'s ruptures and with very rare exceptions are false. The hernial gate can be localized in any department of D., most often in the left dome. Rarely is a traumatic phrenopericardial hernia, usually with prolapse of the omentum into the pericardial cavity, and intercostal diaphragmatic hernia, which occurs when D. is simultaneously damaged in the area of \u200b\u200bthe phrenopericardial sinus and the chest wall, when the abdominal organs through the intercostal space or the area of \u200b\u200bthe damaged rib protrude outward.
Symptoms. In some cases (with wide hernia orifices, gradual and insignificant prolapse of the abdominal organs), diaphragmatic hernias may not show symptoms for a long time.
Their appearance depends on the compression of the lung and the displacement of the heart by the abdominal organs that have fallen into the chest, as well as from the compression and bends of the fallen out organs, in these cases the symptoms are more pronounced with narrow hernia orifices. Accordingly to this, cardiopulmonary, went. - kish. and general symptoms. The most typical complaints are pain in the epigastric region, chest, hypochondrium, shortness of breath, palpitations, vomiting, a feeling of heaviness in the epigastric region after eating. Gurgling and rumbling is often noted in the corresponding half of the chest.
With the volvulus of the stomach, which is often observed in large diaphragmatic hernias, accompanied by an inflection of the esophagus, paradoxical dysphagia is observed, when the swallowed fluid is retained, and solid food passes well. A pronounced wedge, the picture is observed with strangulated diaphragmatic hernias. There is an attack of severe pain and a feeling of compression in the corresponding half of the chest or upper abdomen, often radiating to the back, scapula. Indomitable vomiting appears, at first reflex, and then (with infringement of the intestine) associated with intestinal obstruction. A state of shock often develops. When the intestines are infringed, intoxication develops. Infringement of the hollow organ of the abdominal cavity may be accompanied by its necrosis and perforation with the development of pyopneumothorax (see).
Diagnosis. A presumptive diagnosis of a diaphragmatic hernia is established on the basis of indications of trauma to the abdomen and chest (with traumatic hernias), the above complaints, the definition of dullness or tympanitis over the corresponding half of the chest, changing intensity depending on the filling of the stomach and intestines, listening to intestinal noises in this area ... The final diagnosis is established by rentgenol, research.
Rentgenol, the picture depends on the nature and volume of the displaced organs. When the stomach is prolapsed, there may be a large horizontal level (Fig. 3) in the left half of the chest with the air level above it; with intestinal prolapse - separate areas of enlightenment and darkening. D.'s contours may not be clearly defined. A contrast study of the stomach and intestines allows us to determine the nature (hollow or parenchymal) of the fallen out organs, to clarify the localization of the hernial orifice (Fig. 4) on the basis of compression of the displaced organs at the level of the opening in the D. (symptom of the hernial orifice).
It is most difficult to differentiate hernia and relaxation of D. However, there is a number of rentgenol, signs that allow this.
Treatment... The established diagnosis of diaphragmatic hernia in connection with the possibility of infringement is an indication for surgery, with the exception of sliding hiatal hernias D., in which there is no infringement.
Anesthesia - endotracheal anesthesia with the use of muscle relaxants (see). The choice of access depends on the side of the lesion, the localization of the hernial orifice and the nature of the hernia. With rare right-sided localization, the operation is possible only through transthoracic access to the IV intercostal space. With parasternal hernias, both on the right and on the left, the best access is the upper median laparotomy. (cm.). With left-sided hernias, due to the possibility of adhesions with the lung, which are difficult to separate during laparotomy, a transthoracic approach is shown in the VII-VIII intercostal space with the intersection of the costal arch. However, in cases of congenital posterolateral defects of D., access below and parallel to the costal arch can be successfully applied. The operation consists in separating the adhesions of the prolapsed abdominal organs with the lung and in the area of \u200b\u200bthe hernial orifice. Particular care should be taken when spleen prolapse, damage to a cut usually forces splenectomy (see).

After separation of adhesions and complete release of the edges of the defect, the fallen organs are brought down into the abdominal cavity and the defect is sutured. In the overwhelming majority of cases, this is possible by imposing separate sutures with the formation of a duplication. Often, with traumatic hernias, the edges of the D. are tucked up and grow together with the chest wall, which creates the impression of a complete absence of D. Isolation of the edges of the defect allows them to be straightened and sewn. If this fails, one has to resort to a number of techniques, for example, D. mobilization, in particular, by dissecting the phrenic-costal sinus. It is possible to use alloplastic strengthening of D. with a fabric made of polymers, which is sewn to D. as a patch from the inside, and the edges of the defect are sewn over it (Fig. 5). If this is not possible, the patch is sewn over the gap. In case of lateral defects due to D.'s separation, its edge is fixed to the intercostal space fabric; for large defects, they resort to alloplastic strengthening (Fig. 6), and the tap of the fabric is sewn in such a way that it goes 1.5 cm beyond the edge of D.
With parasternal hernias, after bringing down the displaced viscera, the hernial sac is inverted and cut off at the neck. Then on the edges of D. and the posterior leaf of the sheath of the abdominal muscles, as well as the periosteum of the sternum and ribs, sutures are applied (Fig. 7), usually U-shaped, which are sequentially tied.
Posterior-lateral defects are sutured transabdominally with separate sutures with the formation of a duplication and leaving the drainage introduced through D.
Operations for restrained diaphragmatic hernias have their own characteristics. Access for restrained diaphragmatic hernias, installed before the operation, must be transthoracic. Therefore, in those cases when a restrained diaphragmatic hernia is found during a laparotomy for an acute abdomen, a considerable time after the infringement, it is advisable to switch to thoracotomy (see) in order to avoid the threat of rupture of the restrained organ and not infect the abdominal cavity. In the absence of pronounced necrotic changes, the restraining ring is first dissected along the grooved probe and the state of the restrained organ section is examined. With confidence in its viability, the fallen organ is immersed in the abdominal cavity and the defect is sutured in D., which usually does not cause difficulties in connection with the narrow hernial orifice. In case of irreversible changes, the affected department is resected, and then D. is sutured, leaving the drainage in the pleural cavity.

Hernia of the esophageal opening of the diaphragm can be sliding (axial) and paraesophageal (Fig. 8). Sliding hernias half a mile their name because when the cardia moves along the axis of the esophagus above D., the cardial part of the stomach, due to the mesoperitoneal position, takes part in the formation of the wall of the hernial sac. Sliding hernias (Fig. 8, 2, 3, 9-12) of the esophageal opening of D. are divided into esophageal, cardiac, cardiofundal, and giant (subtotal and total gastric hernias, in which the stomach turns in the chest). A sliding hernia can be fixed and non-fixed, congenital and acquired. In addition, due to the peculiarities of the anatomy, clinic and treatment, the acquired short esophagus I and II degrees and the congenital short esophagus (pectoral stomach) are isolated, associated with its exclusion into the abdominal cavity during the embryonic period. The blood supply to the thoracic stomach in these cases is carried out from the branches of the intercostal arteries.
With paraesophageal hernias, the stomach or intestines are displaced through D.'s esophageal opening next to the esophagus, while the cardia remains in place.
This, in contrast to sliding hernias, leads to the possibility of infringement. Paraesophageal hernias are divided into fundic, antral, intestinal, gastrointestinal, omental hernias by the nature of the organs that have fallen out (Fig. 8, 4-8).
In the development of an acquired sliding hiatal hernia, the main role is played by the reduction of the longitudinal muscles of the esophagus as a result of its irritation, reflex from the stomach and adjacent organs with gallstone disease, ulcers, etc. It is possible to develop a traumatic hiatal hernia after surgery on D. and stomach.
When hiatal hernia there is a straightening of the angle of His, formed between the esophagus and the bottom of the stomach, smoothing of the Gubarev valve (the lip-shaped fold of the mucous membrane at the junction of the esophagus into the stomach) and cardia insufficiency with gastroesophageal reflux occurs (see).
Symptoms... The most common symptom is a burning or dull pain in the epigastric region, behind the sternum and in the left or less often in the right hypochondrium, radiating to the region of the heart, scapula, and left shoulder. The pain intensifies after eating and in the horizontal position of the patient, accompanied by belching, regurgitation, heartburn. Dysphagia is often noted, especially with complications by esophageal stricture, and anemia due to hron, bleeding. Reflex angina pectoris often happens (see).
Diagnosis... The specified complaints and a wedge, symptoms make it possible to suspect a hiatal hernia D. The final diagnosis is established with rentgenol, research, when the continuation of the folds of the cardiac stomach above the diaphragm is noted (Fig. 9) with shortening of the esophagus (or without it), expanded angle of His and reflux of contrast agent from the stomach into the esophagus. Reflux must be checked in a horizontal position of the patient with pressure on the stomach.
With concomitant reflux esophagitis (see. Esophagitis), the esophagus can be expanded and shortened. The radiograph is characterized by the presence of "notches" separating the cardia) from the gastroesophageal vestibule.
For diagnostics, esophagoscopy is also used (see), which allows to examine the state of the esophageal mucosa and to state the presence of reflux esophagitis.
Treatment... For uncomplicated forms of hernia of the esophageal opening D. conservative treatment is shown - the same as for peptic ulcer disease (see). In the absence of achilia, food should be taken in small portions 5-6 times a day. After eating, the patient should not go to bed, the last meal should be at least 3 hours before bedtime. You should not drink plentifully, since it promotes regurgitation (see). Avoid pronounced torso bends and sleep with an elevated upper body. Drug therapy is aimed at reducing secretion (as in a peptic ulcer), at eliminating constipation, including the use of antacids and sedatives.
The indication for surgical treatment is the failure of long-term repeated conservative treatment in patients with pronounced wedge, manifestations of a hernia, as well as complications of a hernia by a peptic stricture of the esophagus and bleeding. A trans-abdominal approach is used, except in cases of extended peptic strictures of the lower third of the esophagus, when transthoracic access is required.
A large number of different surgical methods have been proposed, of which the Nissen fundoplication (Fig. 10), aimed at restoring the valvular function of the cardia, is the most widespread.
After mobilization of the abdominal esophagus, the posterior wall of the fundic stomach is carried out behind the esophagus and sutured to its anterior wall with a two-row suture that captures the esophagus wall. A cuff is formed that surrounds the esophagus, due to which the acute angle of the His is restored. Isolated gastropexy (see), esophagofundoraphy should be left as insufficiently effective. Also, suturing of the esophageal opening is ineffective, since this does not restore the valve function of the cardia, and with a short esophagus, this method is generally not applicable.
When shortening the esophagus to eliminate reflux, valvular gastroplication can be used (according to H.N. Kanshin). In this case, fundoplication is performed not around the esophagus, but around the mobilized cardiac part of the stomach. A number of surgeons use the Collis operation, which consists in dissecting the stomach moved upwards from top to bottom along the esophagus parallel to the lesser curvature by 12-15 cm with lengthening due to the formed gastric tube.
In the treatment of peptic strictures of the esophagus, in case of failure of repeated dilations with special bougies, resection of the narrowed area with valvular esophagogastroanastomosis is indicated.
Paraesophageal hernias give more pronounced symptoms associated with compression of the hernial contents, and the possibility of infringement makes the operation indicated immediately after the diagnosis is made. The operation consists in bringing down the abdominal organs and suturing the hole in D.
For strangulated hernias, the operation is the same as for other diaphragmatic hernias.

Relaxation of the diaphragm - a sharp thinning of D., devoid of muscles, with its displacement together with the abdominal organs adjacent to it into the chest. D.'s line of attachment remains in its usual place. As a rule, there is compression of the lung on the side of the lesion and displacement of the heart in the opposite direction (Fig. 11), there is a transverse and longitudinal volvulus of the stomach, so that the cardia and antrum are at the same level.
Relaxation is congenital (due to aplasia, the muscle is absent) and acquired (most often due to damage to the phrenic nerve; in this case, with histol, D.'s research, remnants of atrophic muscle fibers can be found).
Relaxation is complete (the whole dome is affected, more often the left one) and limited (any part of D. is affected, more often the antero-medial right).
The clinical picture. Limited right-sided anteromedial relaxation is usually asymptomatic and is an accidental rentgenol, a finding. With left-sided relaxation, the symptoms are the same as with a diaphragmatic hernia, but, in contrast to
The latter, due to the absence of hernia orphans, is impossible to infringement. With a gradual displacement of organs, the disease may be asymptomatic.
The diagnosis is made on the basis of signs of displacement of the abdominal organs in the corresponding side of the chest cavity and is confirmed by rentgenol, research. Unlike a hernia, the shadow of a highly located D. is usually clearly defined over the displaced abdominal organs, under a cut the stomach and large intestine give a symptom of open corners. Limited right-sided anteromedial relaxation has to be differentiated. with tumors and cysts of the liver, pericardium and lung.
Treatment. The operation is shown only in the presence of a pronounced wedge, symptoms and consists either in the formation of a thinned D.'s duplication, or in its plastic strengthening using alloplastic materials. For this purpose, ayvalon (a sponge made of polyvinyl alcohol) is suitable, which is sewn in the form of a special patch between the sheets of D.'s duplication along the line of its attachment (Fig. 12).
Diaphragmatic hernia in children occur more often as a result of a malformation of D., less often - as a result of trauma, a purulent-inflammatory or infectious process, therefore they are usually divided into congenital and acquired. Congenital hernias are subdivided into true (Fig. 13, 1-3), having a hernial sac, and false (Fig. 13, 4-6), in which the organs of the abdominal cavity through a through defect D. directly contact the lung and heart. The frequency of congenital D.'s hernias is 1 in 1700 newborns (S. Ya. Doletsky, 1976). The combination of D.'s hernia with other malformations (congenital dislocation of the hip, torticollis, pyloric stenosis, embryonic hernia, heart disease, narrowing of the pulmonary artery, etc.) is observed in 6-8% of cases.
D.'s acquired hernias are divided into traumatic and non-traumatic. The causes of traumatic hernias can be: D.'s ruptures (acute and chronic) and D.'s relaxation (due to phrenic nerve injury). Non-traumatic hernias can occur with through defects of D. (as a result of an abscess located under or above D.) and during D.'s relaxation (after poliomyelitis or tuberculosis).
Hernias of the esophageal opening D. (Figs. 13, 7 and 8) in children develop due to a slowdown in the rate of lowering of the stomach from the chest cavity to the abdominal cavity and the absence of obliteration of the air-intestinal pockets, resulting in the appearance of hernial sacs. Congenital hernias of D., including with its slit-like defects, as well as phrenopericardial hernias (Figs. 13, 9 and 10) occur in the anatomically "weak" parts of D. - the sternocostal gap, lumbar triangle, etc. Formation of thinned zones or through defects D. occurs in the early stages of development of the embryo and fetus. Violation of trophic processes in D.'s muscular anlage leads to a slow pace of D.'s development, increased intra-abdominal pressure in comparison with intrapleural pressure - to the introduction of the abdominal organs into the chest, which occurs in the last weeks of intrauterine life. D.'s postnatal development is accompanied by its relative atrophy in connection with the increasing value of the function of the intercostal muscles. The sterno-costal and lumbar-costal triangles progressively decrease, the area of \u200b\u200bthe tendon center increases due to the muscular sections. D.'s weight decreases relative to the weight of the whole body.
D.'s acquired hernias arise as a result of open or closed trauma. Often D.'s rupture with the subsequent development of a traumatic diaphragmatic hernia occurs with a fracture of the pelvis due to a sharp increase in intra-abdominal pressure. Tuberculous bronchadenitis and a nonspecific inflammatory process in the mediastinum can be complicated by damage to the phrenic nerve with atrophy of part or all of D.'s dome and the development of its relaxation. With a subphrenic abscess or a decubitus, as a result of prolonged drainage of the pleural cavity, a defect may form in D. with subsequent movement of the abdominal organs into the chest.
The clinical picture. In newborns with a slit-like defect in the posterior part of D. (Bochdalek's triangle), cyanosis, vomiting, displacement of the heart, and a scaphoid sunken abdomen ("asphyxia") are observed. When a significant volume of the abdominal organs is moved to the chest, there is a lag in the development of the child, shortness of breath when running, deformation of the chest. With a hernia of the esophageal opening, anemia, vomiting with an admixture of blood, pain, and the phenomenon of erosive esophagitis are noted. In some cases, diaphragmatic hernias may be asymptomatic (or with an unusual combination of common symptoms). They are detected during rentgenol, chest examination, carried out for another reason.
Infringement of a diaphragmatic hernia is characterized by a combination of signs of intestinal obstruction and respiratory failure (see).
Diagnosis. A history of trauma or scars on the skin of the chest contributes to the diagnosis of traumatic diaphragmatic hernia. Physical symptoms in the areas of hernia projection (shortening of the percussion sound or tympanitis, intestinal noises, splashing, etc.) give grounds to suspect a diaphragmatic hernia and make rentgenol. research to establish the final diagnosis. Roentgenol, signs of diaphragmatic hernia are the disappearance of D.'s contour ("boundary line"), its characteristic deformation, individual darkening and clarification of the pulmonary field, levels in the cavities, "symptom of variability" is an essential sign of rentgenol. pictures with repeated studies. In doubtful cases, make a contrast study went. - kish. path.
In newborns, the differential diagnosis is carried out with D.'s paresis in connection with a birth injury. With paresis, D.'s dome after 1 - 2 months. is in the correct position. In some cases, due to the displacement of the heart to the right and cyanosis, an erroneous diagnosis of dextrocardia or heart disease is made. Rentgenol is of decisive importance in diagnostics. chest examination.
Treatment is prompt. The exception is limited relaxation and complete relaxation of D. when its dome is located not higher than the IV rib and small hernia of the esophageal opening, provided that in all cases there are no complaints, patol, deviations, developmental delay. In the presence of pain, vomiting, recurrent intestinal obstruction, went. - kish. bleeding, surgery is indicated in an institution where there is experience in such interventions in children. An emergency operation is performed in case of asphyxia in a newborn, in case of D.'s rupture and D.'s strangulated hernia of any localization.
The operation is more often performed by transabdominal access under intubation anesthesia (see. Inhalation anesthesia). In true D.'s hernias, the hernial sac is sutured with collecting sutures or with the creation of a duplication. Excision of the hernial sac is not necessary. In case of slit-like and significant D.'s defects, the introduction of air into the pleural cavity through the hernial orifice using a metal catheter contributes to the reduction of organs.
D.'s defects are sutured with one row of interrupted non-absorbable sutures. For phrenopericardial hernias and significant hernial orifices, the defect is replaced with an alloplastic material (aivalon, Teflon, nylon), with the obligatory delimitation of the latter from the pleural or pericardial cavity with a leaf of the peritoneum on the pedicle, fascia or omentum. Excision of the hernial sac with anterior and paraesophageal hernias is not necessary; the peritoneum is dissected along the perimeter of the hernial orifice in order to sew the deserted tissue. The success of the operation is associated with the movement of the esophagus into the anterolateral part of the esophageal opening, suturing of D.'s legs behind the esophagus, in front of the aorta, creating an acute esophageal-gastric angle by fixing the abdominal segment of the esophagus to the stomach and fixing the fundus of the stomach to the diaphragm in the area of \u200b\u200btheir natural contact. The operation is completed by pyloroplasty in order to avoid persistent vomiting caused by pylorospasm (see) due to trauma to the vagus nerves. In newborns with a small volume of the abdominal cavity, which does not contain the organs brought down from the pleural cavity, the first stage is to create an artifical (artificial) ventral hernia, which is eliminated within 6 days to 12 months. after the first operation. Drainage of the pleural cavity in newborns is performed according to Bulau (see Bulau drainage), avoiding forced expansion of the lung and the occurrence of acute emphysematous pneumonia. Drainage can be carried out below the XI -XII rib transabdominally in order to avoid kinking when the lung is expanded.
Postoperative complications are observed in more than 50% of operated children. Distinguish between general complications (hyperthermia, depression of the respiratory center, violation of water-salt metabolism), pulmonary (atelectasis, edema, pneumonia, pleurisy), abdominal (dynamic and mechanical intestinal obstruction), as well as an excessive increase in intra-abdominal pressure (see), accompanied by restriction D.'s excursions and a syndrome of compression of the inferior vena cava (see. Hollow veins). Recurrences are most often seen in paraesophageal hernias.
Mortality after surgery for diaphragmatic hernias in children is 5-8% (in newborns - up to 10-12%).
Diseases
Symptoms of D.'s diseases are associated with a change in her position (high standing, relaxation, tumors) or the movement of the abdominal organs into the chest with diaphragmatic hernias.
Depending on the predominance of a wedge, manifestations, these symptoms can be divided into three main groups: general, cardiopulmonary, went. - kish. These symptoms are not specific, they can be observed in some other diseases and acquire diagnostic value only with certain objective data.
Inflammation of the diaphragm - diaphragmatitis (or diaphragmites) are divided into acute and chronic, specific and non-specific. In the overwhelming majority of cases, they are secondary. Chron, diaphragmatitis is usually specific - tuberculous, syphilitic or fungal (actinomycosis) and an independent wedge, do not matter, as well as hron, non-specific diaphragmatitis associated with hron, inflammatory processes of adjacent organs.
Acute nonspecific diaphragmatitis is almost always secondary and only rarely depends on the hematogenous spread of infection from distant purulent foci. In the overwhelming majority of cases, it occurs with acute pleurisy and lower lobe abscesses of the lung or with subphrenic abscesses.
Wedge, manifestations of acute diaphragmatitis fit into the diaphragmatic symptom complex described by MM Vicker: sharp pains in the lower parts of the chest, corresponding to the place of D.'s attachment, tenderness in this zone on palpation, local stiffness of the abdominal muscles. V.I.Sobolev (1950) considers a characteristic sign of acute diaphragmatitis to be high standing of the affected dome of D. with limitation of its mobility and flattening, shortening of sinuses, thickening of D.'s contours in the presence of changes from the adjacent lung or subphrenic space. Since such diaphragmatitis is secondary, treatment is aimed at eliminating the main process. The existence of acute primary diaphragmatitis in the literature is disputed, a wedge, they do not matter.
Also rare are primary tumors of D. According to B.V. Petrovsky, N.N. Kanshin and N.O. Nikolaev (1966), 68 primary tumors of D. are described in the world literature: 37 benign (lipomas, fibrolipomas, fibromas, leiomyomas , neurofibromas, lymphangiomas) and 31 malignant (of which 24 are sarcomas, and the rest are hemangio- and fibroangioendotheliomas, hemangiopericytomas, mesotheliomas, synoviomas). In subsequent years, only a few observations were described.
Symptoms depend to a certain extent on the size and location of the cyst or tumor.
At small tumors and D.'s cysts, symptoms are practically absent. When the tumor is large, there may be signs of compression of the lung and displacement of the mediastinal organs with the development of the phenomena of hron, hypoxia (see), the symptom of "drumsticks" (see Drum fingers), and with large right-sided cysts and tumors there are symptoms from the chest organs cells, and with left-sided - they are mainly caused by compression of the abdominal organs or the esophagus. At secondary cysts and tumors germinating in D. from the side of adjacent organs, and at metastatic lesions, there are pains and symptoms determined by the main patol, process.
Diagnosis of primary tumors and D.'s cysts of hl. arr. X-ray and is based on the detection of a round shadow, merging with the shadow of D., in benign tumors. Benign tumors and cysts of the left dome are clearly visible against the background of a lung, deformed gas bubble of the stomach or splenic angle of the colon, and with right-sided localization they merge with the shadow of the liver, which makes differentiate them with right-sided limited relaxation D., tumors and cysts of the liver or similar formations in the lower lobe of the lung.
In these cases, diagnostic pneumoperitoneum or pneumothorax can be used.
With malignant tumors infiltrating D., there is no clear delineation of the formation, there is only a thickening and deformation of the dome, which in some cases are masked by pleural effusion.
Treatment. The established diagnosis of a primary cyst or D.'s tumor is an indication for surgery, which is carried out, as a rule, transthoracally. The operation consists in exfoliation of a benign cyst or D.'s tumor or in its excision within healthy tissues (with suspicion of a malignant character) with subsequent suturing of D.'s defect with separate silk sutures. With a large defect formed after tumor removal, one or another plastic method can be used to close it.
Removal of secondary tumors and D.'s cysts is carried out in cases where it is possible, according to the same principles simultaneously with removal of the main focus.
Summary data on D.'s injuries and main diseases are given in the table.
Table. Classification and clinical and diagnostic characteristics of some injuries and diseases of the diaphragm
|
Damage to disease |
Etiology and pathogenesis |
Symptoms |
Special research |
X-ray symptoms |
Therapeutic |
|
Damage |
|||||
|
Closed (direct, indirect, spontaneous) |
Most often - road and work injury, falling from a height, compression; is often a component of associated trauma. A gap of 90-95% is localized on the left. Through the resulting defect, the abdominal organs are displaced into the chest cavity, forming an acute diaphragmatic hernia. Displacement of organs can occur at the time of injury or much later. |
Pain in the upper abdomen and the corresponding half of the chest radiating to the supraclavicular region, neck, arm. Dyspnea. Cyanosis. Tachycardia. Phenomena of partial intestinal obstruction are possible. Displacement of dullness of the mediastinum to the healthy side. Tympanitis or dullness within the pulmonary field. Variability of percussion and auscultation data. Detection of a diaphragm rupture during laparotomy in a patient with abdominal trauma (a gap of 90-95% is localized on the left) |
Fluoroscopy and X-ray of the chest and abdomen. If the patient's condition allows, examination of the stomach and intestines with a barium suspension. If diagnosis is difficult - diagnostic pneumoperitoneum |
Raising the level of the diaphragm, limiting its mobility, sometimes deformation of the dome; accumulation of fluid (blood) in the costo-diaphragmatic sinus. With prolapse of the abdominal organs - darkening of the pulmonary field with enlightenments, sometimes with horizontal fluid levels. Displacement into the chest cavity of the contrasting stomach or intestinal loops |
Treatment is prompt. Access - thoracotomy or laparotomy. After releasing the displaced organs into the abdominal cavity, suturing the rupture of the diaphragm with sutures made of non-absorbable material |
|
Open (stab-cut, gunshot) |
A mandatory component of any thoracoabdominal injury |
The severity of the patient's condition is due to the combined damage to the organs of the chest and abdomen, pneumothorax, shock, bleeding. There are three types of clinical presentation: 1) the predominance of symptoms from the abdominal organs (bleeding, peritonitis); 2) the predominance of symptoms from the organs of the chest cavity (hemothorax, pneumothorax); 3) equally expressed symptoms from the organs of the chest and abdominal cavity. Loss of abdominal organs into the wound or the expiration of their contents, pneumo- and hemothorax in the wounded in the abdomen, symptoms of hemoperitoneum or peritonitis with chest wounds |
Fluoroscopy and chest X-ray. Thoracocentesis or laparocentesis. In difficult cases, diagnostic pneumoperitoneum. Examination of the stomach and intestines with barium suspension is contraindicated |
Detection of pneumo- and hemothorax in abdominal injuries, as well as symptoms of closed diaphragm injuries |
Revision of the abdominal organs, elimination of their possible damage. Suturing damage to the diaphragm, eliminating hemo- and pneumothorax, draining the pleural cavity |
|
Foreign bodies |
Blind wounds (especially multiple shrapnel and shot wounds) |
Specific, as a rule, absent or may correspond to the symptoms of diaphragmatitis |
Roentgenokymography, diagnostic pneumoperitoneum and pneumothorax |
Moving the shadow of a foreign body during breathing together with the diaphragm, especially in conditions of diagnostic pneumoperitoneum and pneumothorax |
With prolonged existence and the absence of symptoms, surgical treatment is not? shown. For newly penetrated sharp foreign bodies (e.g. needles) and symptoms of suppuration: removal by thorapotomy is indicated |
|
Acute diaphragmatitis |
|||||
|
nonspecific secondary |
Transition of infection to the diaphragm with pleurisy, lung abscess, subphrenic abscess, liver abscess, peritonitis |
A triad of signs: 1) pain in the lower parts of the chest, aggravated by inhalation, coughing, but not by movement; 2) when pressing in the intercostal space, the pain in the zone of pain distribution does not increase; 3) the rigidity of the muscles of the anterior abdominal wall. Auscultation may cause pleural rubbing noise. Fever, intoxication |
Radiography, tomography, roentgenokymography. If pleural empyema is suspected, diagnostic puncture |
Flattening, high standing and blurred contours of the affected dome of the diaphragm with a sharp limitation or lack of mobility (sometimes paradoxical movements). Accumulation of fluid in the costophrenic sinuses. In appropriate cases, lower lobe pneumonia, signs of liver abscess, subphrenic abscess |
Conservative or surgical treatment: of the underlying disease |
|
nonspecific primary |
Hematogenous or lymphogenous penetration of the pathogen into the thickness of the diaphragm |
Same as for secondary diaphragmatitis |
Usually conservative antibacterial and anti-inflammatory treatments |
||
|
Chronic diaphragmatitis |
|||||
|
nonspecific |
The consequence of the postponed acute diaphragmatitis, less often primary chronic lesion |
The same as with the residual effects of pleurisy: chest pain, aggravated by inhalation, moderate shortness of breath, dry cough |
Higher standing of the affected area of \u200b\u200bthe diaphragm with flattening and deformation, with indistinct contours, limited adhesive process, limited and sometimes paradoxical movements |
Anti-inflammatory treatment, physiotherapy |
|
|
specific |
Tuberculosis, syphilis, fungal infections (actinomycosis) |
Same as in acute diaphragmatitis |
Same as for nonspecific diaphragmatitis |
Specific |
|
|
Corresponds to similar cysts of other sites |
They are associated with the nature, size, localization of education and depend mainly on the compression of the adjacent organs. With large formations - local dullness, weakening or absence of respiratory sounds. With echinococcosis - eosinophilia, positive Casoni reaction |
Radiography, tomography, diagnostic pneumothorax and pneumoperitoneum. Ultrasonic location |
The cysts of the left dome of the diaphragm are visible against the background of gas-containing organs (lung, stomach, splenic angle of the colon). With right-sided localization, they merge with the shadow of the liver |
Surgical removal (thoracotomy) |
|
|
Benign |
The origin and structure correspond to benign tumors of other localizations. Rare |
Same as for cysts |
|||
|
Malignant (primary - sarcomas, synoviomas; secondary) |
Primary tumors are rare, secondary ones are frequent (metastases of cancer of the lung, stomach, liver, etc.) |
A combination of symptoms of diaphragmatitis and diaphragm cysts. In secondary tumors, symptoms of the underlying disease, often symptoms of pleural exudate |
In the presence of pleural exudate - puncture and cytol, punctate examination, thoracoscopy |
Often the presence of symptoms of pleural exudate. Other symptoms like cysts |
In primary malignant tumors - resection of the dome of the diaphragm with simultaneous plastic surgery. For secondary - treatment of the underlying disease |
|
Diaphragmatic hernia |
|||||
|
Traumatic (false hernia) |
|||||
|
acute, chronic |
The consequence of open and closed damage to the diaphragm |
In acute hernia, see Damage; with hron, hernia can be of two types: 1) gastrointestinal (pain in the epigastric region, hypochondrium, chest, radiating upward, emaciation, vomiting); 2) cardiorespiratory (shortness of breath, palpitations, aggravated after eating, with physical exertion). When prolapse into the chest cavity of the stomach, gastric bleeding is possible with the development of anemia; dullness of percussion sound or tympanitis over the pulmonary field; absence or weakening of breathing sounds, rumbling, peristaltic murmurs, splashing noise on auscultation of the chest |
Fluoroscopy and X-ray of the chest and abdomen. According to indications - research went. - kish. tract with barium suspension. Diagnostic pneumoperitoneum |
Depends on which organs are moved to the pleural cavity. When the stomach is displaced, there can be a large horizontal level in the pleural cavity with the air level above it. When the intestine is displaced, separate areas of enlightenment and darkening. The contours of the diaphragm may not be clearly defined. Case study clarifies the nature of the displaced organs |
Surgical treatment is indicated |
|
restrained |
The same as for entrapment of ventral hernias |
Sharp pain in the chest and upper abdomen; vomiting, shortness of breath, palpitations, often shock; with intestinal infringement - signs of intestinal obstruction. Subsequently - growing intoxication |
Radiography, including in lateroposition. Examination of the stomach and intestines with barium suspension |
Signs of hernia and signs of compression of the prolapsing organ in the hernial orifice |
Emergency operation. Access is determined by "the localization of the hernia, the size of the defect, the condition of the patient |
|
Non-traumatic |
|||||
|
false congenital hernias (birth defects) |
Diaphragm malformation, mainly in children |
In most patients, symptoms (cyanosis, shortness of breath, vomiting) occur from the moment of birth. In the future, the lag in physical is added. developmental disorder, poor appetite |
Diagnostic pneumoperitoneum |
See Traumatic diaphragmatic hernia. |
Surgical treatment is indicated |
|
True hernias of weak areas of the diaphragm (parasternal, lumbocostal hernia of Bohdalek) |
Congenital large gaps between the anatomical parts of the diaphragm, increased intra-abdominal pressure |
Depends on the nature and volume of the hernial contents. For small hernias, symptoms may be absent |
For differential diagnosis between the hernia and the parasternal wen, pneumoperitoneum and the introduction of air into the preperitoneal tissue are used |
Same as for traumatic diaphragmatic hernias |
Surgical treatment is indicated |
|
Sliding hiatal hernia (cardiac, subtotal gastric and total gastric) |
Increased intra-abdominal pressure and longitudinal contraction of the esophagus, as well as constitutional weakness of the interstitial tissue. Through the dilated esophageal opening of the diaphragm, the cardia with more or less of the stomach is displaced into the mediastinum |
Pain and burning in the epigastrium and behind the breastbone, heartburn, belching with air, regurgitation, sometimes intermittent dysphagia. Most pronounced with high acidity and shortening of the esophagus. Of great diagnostic value is the intensification of symptoms after eating, in a horizontal position, with bending of the body. Never prejudiced. Vomiting mixed with blood. Anemia |
Esophagoscopy (to exclude cancer of the esophagus and cardiac part of the stomach), esophagomanometry |
Revealed by contrast examination of the esophagus and stomach on a trochoscope |
Surgical treatment is indicated for large sliding hernias with pronounced wedge, manifestations, occasionally with cardiac hernias, accompanied by severe reflux esophagitis (especially ulcerative and stenosing), resistant to conservative therapy |
|
Paraesophageal (fundic, antral, intestinal, omental) |
Congenital non-closure of embryonic recessus pneumatoentericus. The fundus of the stomach, its antrum, intestinal loop or omentum, covered with a hernial sac, prolapse into the mediastinum next to the esophagus while maintaining the subphrenic location of the cardia. Rare |
Periodically, there is pain high in the epigastrium. Bleeding from the stomach with the development of anemia is possible. In case of infringement - an attack of sharp pain with the development of dysphagia due to compression of the esophagus in the hernial orifice |
Same as for hiatal hernia |
Contrast examination of the esophagus and stomach. Fundal hernia from sliding cardiofundal is distinguished by subphrenic location of the cardia |
Surgical treatment is indicated |
|
Rare hernias of natural openings of the diaphragm (hernia of the cleft of the sympathetic trunk; hernia of the opening of the inferior vena cava; hernia of the opening of the intercostal nerve) |
Congenital enlargement of the named holes. Hernias are true. Very rare |
They have no specific symptoms. Clarification of the nature of the hernial orifice is possible only during surgery or autopsy |
Surgical treatment is indicated |
||
|
Relaxation |
With congenital relaxation - underdevelopment of the muscular elements of the diaphragm; when acquired - their atrophy due to inflammatory changes or damage to the phrenic nerve. The thinned dome of the diaphragm (or its section) is displaced high upward, causing collapse of the lung, displacement of the mediastinum, upward movement of the abdominal organs, compression of the lung |
Pain in the epigastrium or hypochondrium, shortness of breath, palpitations, feeling of heaviness after eating, belching, nausea, constipation, weakness. Recurrent pneumonia of the lower lobe localization |
Diagnostic pneumoperitoneum |
High standing of one of the domes of the diaphragm or part of it. Paradoxical movement of the corresponding dome ("swing symptom") or limitation of mobility during partial relaxation. Partial relaxation requires differential diagnosis with tumors (cysts) of the lung, diaphragm, liver |
Surgical treatment is shown in Ch. arr. with total relaxation with the expressed wedge, manifestations. With partial relaxation, the operation is indicated if it is impossible to exclude a tumor of the diaphragm or liver |
Bibliography: Bairov GA Emergency surgery of children, L., 1973; Doletsky S. Ya. Diaphragmatic hernias in children, M., 1960, bibliogr .; Nesterenko Yu. A., Klim and a certain IV and Lelekhova NI Ruptures of the right dome of the diaphragm, Surgery, No. 4, p. 106, 1975; Petrovsky BV, Kanshin H. N. and Nikolaev N. O. Diaphragm surgery, L., 1966, bibliogr .; V. V. Utkin and Apsitis BK Hernias of the esophageal opening of the diaphragm, Riga, 1976; Fekete F., P. et Lortat-Jacob J. L. Ruptures du diaphragme, Ann. Chir., T. 27, p. 935, 1973; H e i m i n g E., E b e 1 K. D. u. G h a r i b M. Komplikationen bei Zwerchfellanomalien, Z. Kinderchir., Bd 15, S. 147, 1974; Koss P. u. R e i t t e r H. Erkrankungen des Zwerchfells, Handb. d. Thoraxchir., Hrsg. v. E. Derra, Bd 2, T. 1, S. 191, B. u. a., 1959; Olafsson G., Rausing A. a. H o 1 e n O. Primary tumors of the diaphragm, Chest, v. 59, p. 568, 1971; Strug B., Noon G. P. a. B e a 1 1 A. C. Traumatic diaphragmatic hernia, Ann. thorac. Surg., V. 17, \\ e. 444, 1974.
B.V. Petrovsky; S. Ya. Doletsky (ped.), Compiler of the table. H. N. Kanshin.